





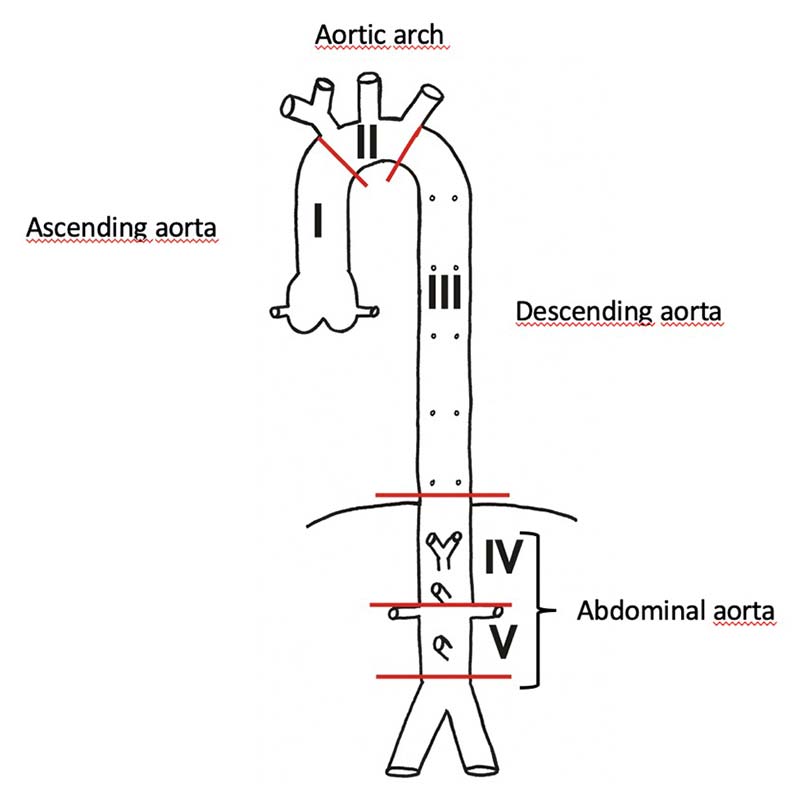
The aorta can be divided into five parts (I-IV). Three of these parts (I-III) compose the thoracic aorta: Ascending aorta (incorporating the aortic valve and the origin of the coronary arteries, which supply the heart), aortic arch (giving origin of the vessels to the head and arms), and descending aorta (with origins of the arteries supplying the spinal cord), respectively (Figure 1).
Diseases of the thoracic aorta include arteriosclerotic processes, dilatations (aneurysms), narrowing (stenosis), inflammatory diseases and tears of the inner and mid layer of the aortic wall, causing an acute, incomplete rupture (aortic dissection). An aortic dissection is a life-threatening disease, generally requiring an emergency operation. In contrast to atherosclerotic processes and/or aneurysmal disease, which are often without any clinical symptoms, patients with an acute aortic dissection typically describe a sudden onset of a sharp pain between the shoulder blades.
Any kind of sudden onset of chest pain requires urgent medical attention!
Tremendous progress has been made in the treatment of diseases of the thoracic aorta. Based on extensive scientific and research work, surgical procedures today are safe and can be performed as less invasive operations for patients.
The Baird Institute is involved in comprehensive basic laboratory and clinical research work, addressing all kinds of aortic surgery.
Surgical principles of aortic surgery consist of replacement of the diseased aorta using a vascular prosthesis. Vascular prostheses basically last forever and are well adopted by the human body without rejection. The operations are performed using the heart-lung-machine and specific protection strategies for the heart, the brain and all other organs. Part of these protection strategies include specific solutions to protect the heart (cardioplegic solution), continuous perfusion of the brain and protection of all organs by cooling the patients on the heart-lung-machine.
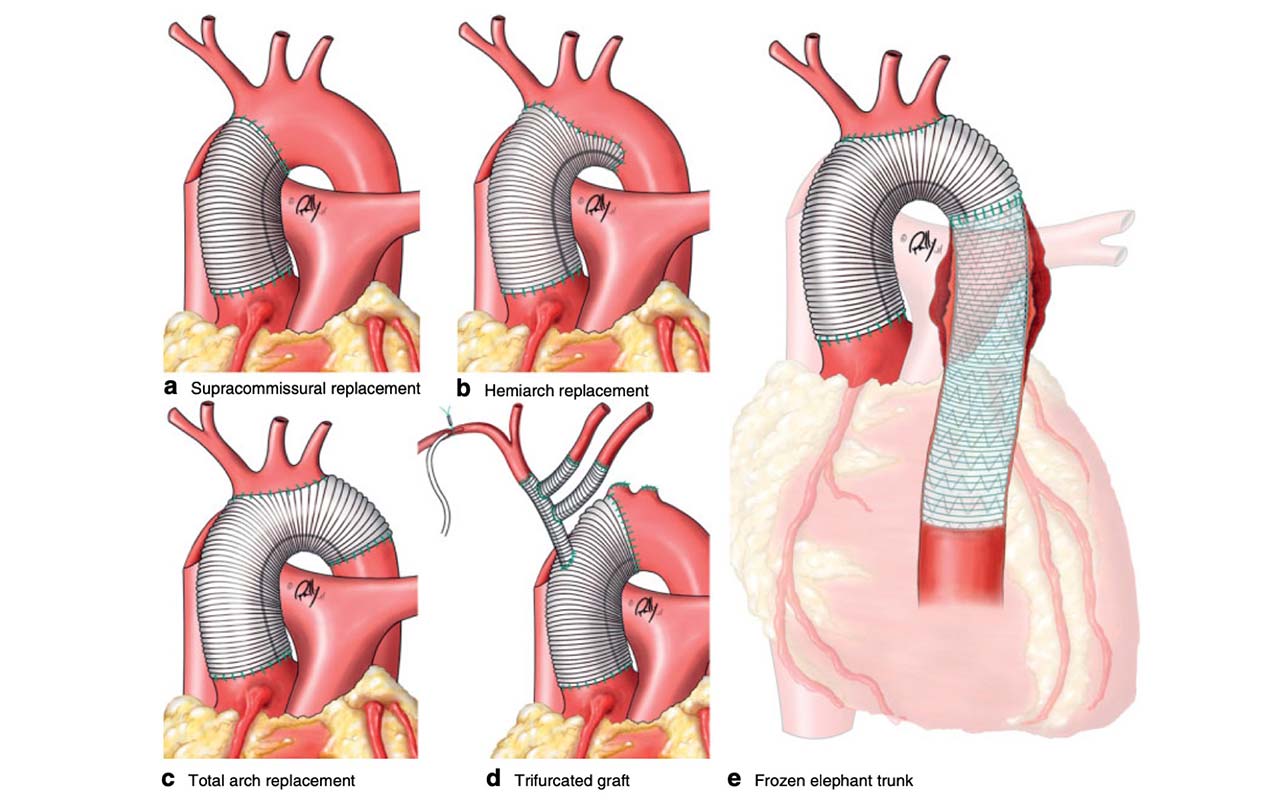
Figure 2 depicts some examples of replacements of parts of the thoracic aorta. These include:
a) SUPRACOMMISSURAL REPLACEMENT:
The ascending aorta is replaced with a vascular graft of appropriate size from above the aortic valve to the aortic arch.
b) HEMIARCH REPLACEMENT:
The ascending aorta and parts of the aortic arch (hemiarch) are replaced.
c) TOTAL ARCH REPLACEMENT:
The ascending aorta and the complete aortic arch are replaced with a vascular graft.
d) TRIFURCATED GRAFT:
The ascending aorta and parts of the aortic arch are replaced. The vessels supplying the head and arms are connected to the aortic graft using a specially designed vascular graft (trifurcated graft).
e) FROZEN ELEPHANT TRUNK:
Almost the whole thoracic aorta is replaced with a so-called hybrid prosthesis. This prosthesis consists of a conventional vascular graft (for the ascending aorta and the aortic arch) and a stent graft for the descending aorta. This special hybrid prosthesis is also called “frozen elephant trunk”, as the original vascular graft, loosely hanging into the descending aorta (“elephant trunk” procedure described by Prof. H. Borst, Hannover Medical School, Germany in 1983), is now replaced by a rigid stent graft (the “frozen elephant trunk”).
It is of importance to note that each surgical procedure is individualized to the patient. This incorporates the design and size of the prostheses used as well as the surgical strategy ie. how much of the aorta has to be replaced, where to connect the heart-lung-machine to the patient, which temperature used, etc.
With today’s modern and innovative surgical techniques, even complex aortic surgery can be performed with a low operative risk.




