




Dr Laurencie Brunel & Prof. Paul Bannon
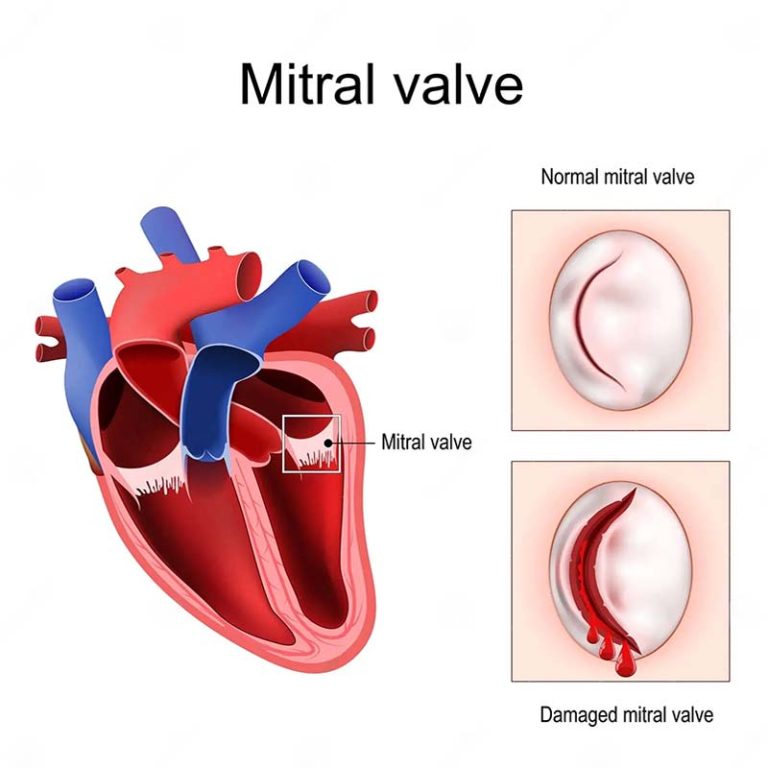
The left side of the heart has 2 chambers (left atrium and ventricle) separated by a valve called the mitral valve. The mitral valve prevents back flow and supports the function of the left ventricle (main pumping chamber of the heart that supplies oxygenated blood to the body and thus essential for life). This valve has two leaflets (anterior and posterior) hinged on the annulus (an ill-defined structure at the junction between the atrium and ventricle).
When the original mitral valve fails to work properly, it can be replaced with an artificial one with the aim of restoring effective blood supply to the body. Valves can be replaced either by opening the chest and heart to insert it (open technique), or by inserting the valve using a minimally invasive approach via a large blood vessel (transcatheter insertion). When the original valve is replaced with an artificial one, there are the options of removing the original one or leaving it in place alongside the new one, or even altering the shape of the original valve. However, all options can severely impair left ventricular function and thus the effective pumping of oxygenated blood to the entire body. Ineffective pumping of blood is a major reason for mortality following valve replacement.
The objectives of our research were to establish a stable and reproducible model to evaluate the effects of commonly used surgical options for the original valve when inserting an artificial valve in clinical practice, with the aim of ultimately improving left ventricular function and therefore quality of life and survival rates of patients requiring a mitral valve replacement.
In current clinical practice, the anterior mitral leaflet is most commonly removed at the time of a valve insertion. Our first study aimed to investigate methods of safely retaining the original anterior leaflet at the time of insertion. This first study found that retaining that leaflet in place, when replacing the valve, caused obstruction in blood flow inside the heart, so clearly, we had to develop other techniques to avoid this.
Some minimally invasive valve replacements are designed to deal with the anterior mitral leaflet, as are some open surgical techniques. So, during our second study we looked at the effects of these techniques on heart function. These studies demonstrated that these methods also adversely affected the heart. Clinically, this at least in part explains the poor outcomes in patients who already have poor heart function going into surgery and in fact we may be making it worse.
We did further investigation into other techniques and the results were all the same. This led us to the conclusion that future designs of any valves, needed to understand that the entire mitral valve apparatus had to be retained, but in some way, we needed to fix the valve function. Hence the importance of this study.




