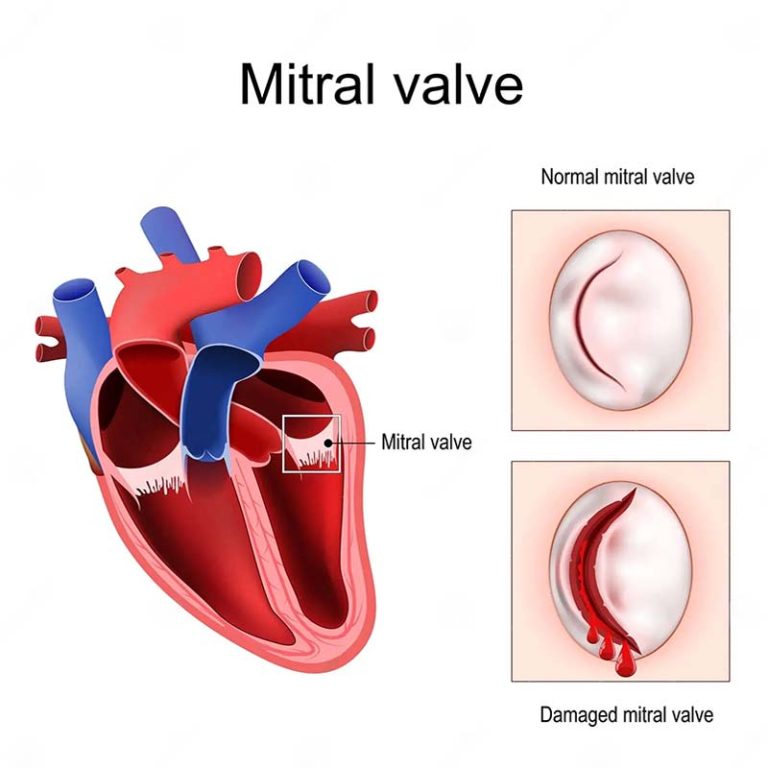
The Role of the Anterior Mitral Leaflet on Left Ventricuclar Function
Dr Laurencie Brunel & Prof. Paul Bannon The left side of the heart has 2 chambers (left atrium and ventricle) separated by a valve called the mitral valve. The mitral valve prevents back flow and supports the function of the left ventricle (main pumping chamber of the heart that supplies oxygenated blood to the body…